
Association of N-terminal telopeptide-1 with BMD in patients with osteopenia and osteoporosis
Aннотация
Background: Osteoporosis is a common disease of aging population, causing fractures and raising mortality and morbidity. Standard diagnosis usually depends on measuring bone mineral density using a dual energy X-ray absorptiometry. But it does not provide information regarding bone formation or resorption. Bone turnover markers provide information regarding bone formation or resorption before the structural changes in bone occur. The aim of the study: This study was undertaken to investigate the effectiveness of N-terminal telopeptide-1 in the diagnosis of osteopenia and osteoporosis. Materials and methods: The case-control study was conducted in 170 individuals from the Department of Orthopedic Surgery. They were divided into three groups based on bone mineral density; group I with normal BMD (n=57), group II with osteopenia (n=62) and group III with osteoporosis (n=51). Institutional ethics committee approval was obtained. Written informed consent was obtained from all the study participants. Serum N-terminal telopeptide-1 (NTX-1) was analyzed by ELISA. Statistical analysis was performed using the SPSS 16.0 version for Windows. The continuous variables were expressed as mean ± SD. ANOVA with Tukey’s HSD and ROC curve analysis were performed. Odds ratio was analyzed. Pearson correlation coefficient was obtained between BMD and NTX1. P value <.05 was considered statistically significant. Results: There was a significant increase in serum N-terminal telopeptide-1 across the groups. NTX-1 values showed correlation with BMD. The area under the curve during analysis of NTX-1 in patients with normal BMD and osteopenia and osteoporosis were 0.697 and 0.592 respectively. Conclusion: The participants were in the obese as well as over-weight category. Serum N-terminal telopeptide-1 was significantly increased across the groups indicating that bone turnover markers are associated with progression of osteoporosis.
Ключевые слова: osteoporosis, osteopenia, bone mineral density, fractures, bone turnover markers, NTX-1
К сожалению, текст статьи доступен только на Английском
Introduction. Osteoporosis is a disease caused by systemic bone loss, the incidence of which increases with age generally affecting one in two or three individuals [1]. About 40% of Caucasian postmenopausal women are affected by osteoporosis, and with an ageing population this number is expected to steadily increase. The lifetime fracture risk of a patient with osteoporosis is as high as 40%, and fractures most commonly occur in the vertebral bones, femur, or wrist bones, also can involve humerus or ribs [2]. It has been estimated that around 40,000, 50,000 and 60,000 vertebral, forearm and hip fractures respectively occur every year in the United Kingdom. Up to 20% of all symptomatic vertebral fractures and 30% of hip fractures occur in men. Although, the incidence of forearm fracture is lower in males than females, men with forearm fractures are at increased risk of vertebral and hip fractures [3].
The skeleton is continually being repaired and remodelled in response to multifaceted stresses. Bone remodelling can decrease bone mineral density (BMD), cortical bone thinning, and increased cortical porosity and trabecular thinning, which may lead to increased bone fragility and increased predisposition to fracture. As the age advances there is increasing osteoclastogenesis, increasing bone marrow adipogenesis, decreasing osteoblastogenesis, decreased osteocyte density and premature osteocyte apoptosis. Bone remodelling is an active and highly regulated process that takes place at a rate of approximately 10-20%, varying by site and type of bone. Postmenopausal osteoporosis involves trabecular bones and is associated vertebral fractures whereas in the elderly men, cortical bone loss occurs with associated hip fracture [1]. The World Health Organisation (WHO) defined osteoporosis in postmenopausal women based on the level of BMD. It is given as a T-score (i.e. standard deviation compared to the mean value of BMD in a young adult women population), of ≤2.5. However, BMD is only one of the contributors of bone strength. Bone fragility depends on numerous factors which together affect micro- and macro-architecture of bone [4]. Bone turnover markers (BTMs) and BMD are independent predictors of fracture risk. Considering the increasing incidence of osteoporosis in aging populations, BTMs need to be measured more easily and economically, as well as accurately and precisely. BTMs seem a better choice for monitoring of early responses to anti-osteoporosis therapy because of the delayed response of BMD to clinical treatment [5].
The aim of the study. This study was undertaken to assess the diagnostic role of N-terminal telopeptide-1 (NTX-1) in patients with osteopenia and osteoporosis.
Materials and methods. The case-control study was conducted in 170 individuals. The study participants of 30-90 years of both sexes were recruited from the Department of Orthopedic Surgery and were divided into three groups based on BMD (measured by DEXA). Group I of 57 individuals (normal BMD), group II of 62 individuals (osteopenia) and group III consisting of 51 individuals (osteoporosis) were included. Institutional ethics committee approval was obtained (IEC-N1/16/JUN/53/36/2016 of 29 June 2016).
This study received funds from the Institutional Founder Chancellor Fellowship. Written informed consent was obtained from all the study participants before they were recruited into the study.
Inclusion criteria: individuals who have undergone DEXA scan for suspected osteoporosis as well as patients with bone fractures in orthopedic department.
Exclusion criteria: Patients with malignancy, stroke, hemi/paraplegia, chronic kidney and liver diseases, rheumatoid arthritis, hyperparathyroidism, thyroid diseases, chronic smokers and alcoholics, bed-ridden / immobile patients, patients on drugs – steroids, bisphosphonates, teriparatide, vitamin-D, calcitonin, immunosuppressants and hormone replacement in females.
Anthropometry measurements such as height, weight, BMI, hip circumference, waist circumference, waist-to-hip ratio & skin fold thickness were taken using standard methods. BMD was determined at the neck of femur and lumbar spine (L1-L4) by DEXA densitometer (GE Lunar Prodigy., Advance Bone Densitometer., US). Based on DEXA T score of BMD, study participants were divided into 3 groups: Group I – Normal bone mass (n=57): T Score = < -1.0 SD; Group II – Osteopenia (n=62) T Score = -1.0 to -2.5 SD; Group III – Osteoporosis (n=51): T Score = > -2.5 SD. Serum NTX-1 was analyzed by ELISA (SiNCERE, catalogue No.:E13650523). Measurement range: 2.54 - 200ng/mL; intra-assay imprecision: <9% and inter-assay imprecision: <15%.
Statistical analysis was performed using SPSS version 16.0 (IBM SPSS, USA) for Windows. The data were found to follow Normal Gaussian distribution. The continuous variables were expressed as mean ± SD. Comparison of independent variables was performed using one-way ANOVA with the Tukey’s HSD post hoc test for identification of differences between specific groups. ROC curve analysis was performed for determination of cut-off value with the corresponding sensitivity and specificity. Odds ratio was analyzed using the Epi Info version 7.2 software (Atlanta, Georgia, USA). Pearson correlation coefficient was used to find association between BMD and NTX-1. P value <0.05 was considered statistically significant.
Results and discussion.
Table 1: Anthropometric Characteristics and serum NTX-1 levels in various study groups
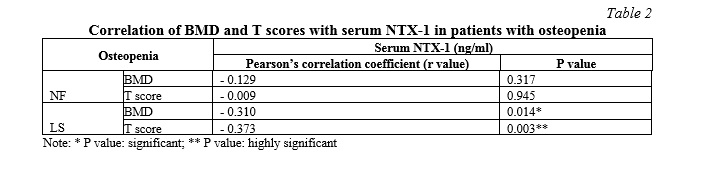
Table 2: Correlation of BMD and T scores with serum NTX-1 in patients with osteopenia
Table 3: Area under the cut-off curve of NTX-1 values in osteopenia and osteoporosis
Figure 1: Receiver Operating Characteristics curve of NTX-1 in osteopenia
Figure 2: Receiver Operating Characteristics curve of NTX-1 in osteoporosis
Discussion. Osteoporosis is a major public health concern, the consequences being fractures, disability, dependence and immobility. As the age advances the bone mass decreases resulting in osteoporosis. The diagnostic criteria by the World Health Organisation (WHO) criterion for osteoporosis is a BMD measurement ≥2.5 SD (T-score ≤ -2.5 SD) below the young female (age 20-29 years) (NHANES III), using the femoral neck as the reference site. Borderline decrease in BMD (T score between -1.0 and -2.5) is designated as osteopenia [6]. Based on BMD, osteoporosis is estimated to be prevalent among 11% of women and 2% of men. Osteopenia is far more frequent, affecting 50% of women and 32% of men. The lifetime fracture risk of a patient with osteoporosis is as high as 40% and fractures most commonly occur in the spine, hip or wrist [7]. In Korea, it was found that in patients with hip fracture 11-17% died within a year while 25% of individuals required long term care. The impact of osteoporosis is projected to increase exponentially due to the rise in the aging population. The worldwide incidence of osteoporotic fractures in 2000 was estimated at 9 million, with hip fractures contributing to 1.6 million. By 2050, the number of hip fractures worldwide is projected to increase to 6.3 million if fracture rates remain constant and Asia is projected to contribute 50% of hip fractures [6]. Osteoporosis is a common cause of morbidity and mortality in adult Indians. In India, about 60 million adults suffer from osteoporosis; 2-3 million fresh cases are added annually. Indians sustain hip fractures occur at an earlier age compared to westerners [8].
In the present study, the mean age of the study participants in the groups I, II and III were 52±13, 52±12 and 55±11 years respectively. The distribution of participants based on gender was almost the same in number across the various study groups. This was indicated by the absence of a statistically significant difference by the Chi-square statistic of 0.27 and P value of 0.87. Individuals who sustained a fracture were included 0%, 4.2% and 7.7% in the groups I, II and III respectively. There was statistically significant Fisher’s exact test with P value of 0.000. As the BMD decreased the number of individuals who sustained fracture increased. There was a statistically significant difference in BMD and T-scores between the groups. The groups were obtained based on the BMD values. Hence, there was a statistically significant difference of P = 0.0001.
In the present study, the statistically significant difference was not observed in BMI. As per Asia-Pacific BMI Guidelines [9], individuals in group I were in the overweight category while individuals in groups II and III were in the obese category. There was a statistically significant difference in waist to hip ratio between the three groups with P value of 0.033. A statistically significant difference was observed between groups I and II, but not when comparing with other groups. Skin fold thickness was measured at the scapular region, triceps region and abdomen. There was a significant decrease in skin fold thickness at triceps region with P value of 0.003. There was a significant difference only between the groups I and III (Table 1). In obesity, aging and diabetes mellitus, the marrow becomes enriched with yellow adipocytes. This leads to dysfunction of the osteogenic and hematopoietic tissues of long bones. The increased marrow adipose tissue (MAT) in obese and individuals is correlated with osteoporosis and increased fracture risk. Similarly, type II diabetes has been linked to reduced bone quality. Marrow adipogenesis is associated with impaired haematopoiesis. MAT accumulation causes the age-related dysfunction of the bone marrow and can be implicated in multiple pathological processes that interfere with appropriate maintenance of bone tissue repair and the hematopoietic system. [10]

Bone loss occurs insidiously and is initially an asymptomatic process, osteoporosis is frequently only diagnosed after the first clinical fracture has occurred. Consequently, therapy is often aimed at preventing further fractures. Therefore, it is important to assess the individual's risk of developing osteoporosis early enough to prevent a first fracture.
Several risk factors such as age, low BMI, previous fragility fractures, a family history of fractures, the use of glucocorticoids and active cigarette smoking have to be taken into account. [2, 11]
Bone turnover markers (BTMs) reflect bone remodelling associated with bone fragility and fractures. Available BTMs are promising fracture risk predictors but there still exists uncertainty regarding their clinical application, mainly due to intra and inter variability of the available assays [7]. The bone markers are also influenced by renal function, diurnal variability, intraindividual variability, stability at room temperature, food intake. This variation is less in blood than in urine [6]. Recent advances show there is better understanding of accuracy, reproducibility, and clinical indications of BTMs. Elevated BTMs, particularly urine resorption markers, are associated with an increased risk of fracture independent of BMD [12]. After the initiation of anti-resorptive therapy, it is easier to measure changes in BTMs compared to BMD, since BMD takes almost a year to show change whereas the changes in BTMs are significant and occur early. Repeat BMD is not advocated within 12 months after initiation of therapy as no significant changes are attained within that time frame. BTMs show a significant change in 3-6 months, hence they can be measured 3 months after initiation of oral bisphosphonates, and bone formation markers 6 months after start of therapy [6].
Bone formation markers are released during the development of osteoblasts. They include bone specific alkaline phosphatase (BSAP), osteocalcin and the carboxy- and amino-terminal propeptides (P1CP, P1NP) [13]. Bone resorption markers are degradation products of bone collagen. Urinary hydroxyproline (OHPr) is a marker of bone resorption. The hydroxy-pyridinium cross links of collagen, pyridinoline (PYD) and deoxypyridinoline (DPD) are formed during the extracellular maturation of fibrillar collagens and are released upon the degradation of mature collagens [14].
In the present study, serum NTX-1 was found to be 219.09 ± 71, 292.1 ± 110 and 300.9 ± 215ng/mL in the groups I, II and III respectively. There was a statistically significant increase with P value of 0.008. The Tukey post hoc test showed that there was a significant increase in serum NTX-1 when group I was compared with groups II or III. But there was no significant difference in sNTX-1 between osteopenia and osteoporosis groups since sNTX-1 in group II is almost the same as that of group III. Hence, serum NTX-1 has a diagnostic as well prognostic role in patients with osteopenia and osteoporosis (Table 1). Serum NTX-1 showed negative correlation with LS -BMD and T score with Pearson’s correlation coefficient of 0.310 and 0.373 and significant P value of 0.014 and 0.003 respectively. But there was no correlation between BMD and T score at the neck of femur and serum NTX-1 (Table 2). The area under the curve during analysis of NTX-1 in patients with normal BMD and osteopenia and osteoporosis were 0.697 and 0.592 respectively (Fig. 1, 2). The cut-off points calculated with Youden index showed that the values for osteopenia and osteoporosis are almost the same showing that NTX-1 could be a better indicator of the stage of osteopenia (Table 3). Odds ratio was found to be 4.6015 with 95% confidence interval of 1.79-11.79 with Z statistics of 3.180 and P value of 0.0015 when analyzed with individuals with normal BMD and osteopenia. Odds ratio was found to be 4.3789 with 95% confidence interval of 1.47-12.99 with Z statistics of 2.661 and P value of 0.0078 when analyzed with individuals with normal BMD and osteoporosis. During bone resorption, cross-linked telopeptides are released from type I collagen, resulting in the formation of N- and C-telopeptides called NTX and CTX, respectively. These telopeptides are increased in few other conditions like Paget’s disease of bone, hyperthyroidism, hyperparathyroidism and other osteolytic lesions of bone. Studies have shown that both urine and serum levels of telopeptides are comparable [15, 16]. Bone formation markers have a negative correlation with BMD and the risk for fracture of long bones [17].



In the process of bone resorption, the amino- and carboxyterminal fragments of collagen are released, with cross-links attached. These fragments with attached cross-links are called telopeptides. N-telopeptides (NTX) and C-telopeptides (CTX/CrossLaps) are excreted in urine. Since more than 90% of the organic matrix of bone consists of type I collagen, measuring its degradation products in urine makes CossLaps a potential specific marker of bone resorption. Several studies have shown that NTXs and CTXs are reportedly specific and sensitive for the resorption of bone tissues, because nonskeletal type I collagen- containing tissues are not actively degraded by osteoclasts and therefore, different fragments are formed in the degradation of other tissues which are comprised of type I collagen. The overall diagnostic efficiency of a single NTX measurement for identifying women with low BMD was 89%. A pronounced and significant increase (47-142%) in CrossLaps at menopause indicates that it is a very sensitive marker of metabolic bone changes taking place at menopause. CrossLaps has a specificity of 80% and a sensitivity of > 70%. [18]
Women on active treatment with alendronate / HRT/ combination therapy, with the greatest decrease in turnover markers (NTX, Bone ALP, osteocalcin (OC)) after 6 months, had the greatest increase in spine and hip bone density after 3 years. Urinary NTX and serum OC provide the greatest sensitivity and specificity for change in bone density, with either calcium supplementation or hormone replacement therapy. Short-term changes in biochemical markers of bone turnover have been suggested as predictors of long-term response in bone mass during antiresorptive therapy. The bone markers predicted a change in spine BMD with a high positive predictive value and specificity [8]. In urinary NTX/creatinine, the reported analytical variability is 8%. An evaluation of both short term and long term intrasubject variability in this study indicates that the day to day and month to month CV is 18–19%, respectively. This measure of variability includes the analytical CV because samples from the same individual were measured separately and not necessarily in the same assay. No association between age, lifestyle factors, or baseline urinary NTX/creatinine and either short term or long term urinary NTX/creatinine was observed [5]. Serum BSAP and the bone resorption markers, urine NTX and serum CTX, were significantly higher (25 to 40%) in postmenopausal women compared with premenopausal women. BMD was also significantly lower in the lumbar spine, femoral neck, total hip, and greater trochanter in postmenopausal women [5].
Conclusion. BMD is the gold standard for assessing the presence of osteoporosis. Serum N-terminal telopeptide-I was significantly increased in individuals with decreased BMD, indicating the use NTX-1 as a bone turnover marker in assessing osteopenia / osteoporosis.
Limitations of the study. This study could have been done with few more bone turnover markers. Sample size could be bigger. If the study is done as a cohort study, time of onset of osteopenia and osteoporosis can be identified early to initiate preventive measures.
Financial support
This study was the major work of Dr P Modagan which was part of his PhD program. This study was partly funded by the Institutional Founder Chancellor Fellowship programme. Other than this the project/publication of the research did not receive any other funding from national or international agencies.
Благодарности
The authors wish to thank the management of Sri Ramachandra Institute of Higher Education and Research for supporting the PhD programme in the form of provision of funds as well as providing necessary infrastructure to conduct the study














Список литературы
Список использованной литературы появится позже.