
Impact of the angiotensin-converting enzyme 2 gene polymorphism on essential hypertension in the southern region of Bangladesh
Abstract
Background: Hypertension (HTN) is a major global health issue influenced by genetic, environmental and demographic factors. The angiotensin-converting enzyme 2 (ACE2), important for blood pressure regulation, has been linked to HTN in different ethnic populations, but research among the southern Bangladeshi population is unavailable. The aim of the study:This study aimed to evaluate the impact of the ACE2 gene G8790A polymorphism on essential HTN, considering epidemiological factors and gender-specific association. Materials and methods: A case-control study was conducted with 260 hypertensive and 234 healthy individuals from Chittagong Medical College, Bangladesh, to genotype the ACE2 G8790A polymorphism by the PCR-RFLP method. Physical, epidemiological and biochemical parameters were assessed to understand their relationship with genetic variations. Results: The study revealed a significant association between the ACE2 AG heterozygous genotype and HTN in females (OR = 15.44, 95% CI 3.56–67.02, P < 0.001) with no similar risk in males (P = 0.742). No significant correlation was identified between the ACE2 polymorphism and biochemical factors. HTN patients had significantly higher levels of serum creatinine (male: 25.11% vs 1.30%; female: 23.97% vs 0%; P < 0.001) and urine albumin (male: 3.40% vs 0%; female: 5.70% vs 0%; P < 0.001) than controls. The low level of HDL cholesterol was noted in HTN patients (male: 49.00% vs 24.78%, female: 48.40% vs 10.25%; P < 0.001). Conclusion: HTN patients with ACE2 gene mutant variants (AG and AA) showed a higher prevalence of diabetes and CVD. This is the first study to highlight a significant gender-specific association between the ACE2 G8790A heterozygous genotype and HTN in Bangladeshi women, offering a potential gender-based biomarker for managing HTN
Introduction. Hypertension (HTN) is a complex medical condition and a major public health issue, affecting about one-third of the global population. Essential hypertension (EH) is a multifactorial and polygenetic disease characterized by increased arterial blood pressure (SBP ≥140 mmHg/DBP ≥ 90 mmHg) frequently stemming from heightened resistance due to arterial constriction, including 90-95% of the HTN cases [1, 2, 3]. Moreover, EH is a pivotal risk factor for myocardial infarction, vascular disease, heart failure, stroke, and renal complications [4]. Despite lifestyle adjustments and treatment options, the incidence of EH is increasing alarmingly and is expected to reach ~29% of the global adults by 2025 [5]. According to the World Health Organization report [6], about 1.28 billion adult individuals suffer from HTN globally, with the majority comprising two-thirds residing in low- and middle-income nations. In Bangladesh, around 68% of fatalities result from non-communicable diseases (e.g., HTN, cardiovascular diseases, diabetes), and HTN contributes to 15-20% of these cases [7].
Essential HTN prevalence and its related complications are attributed to genetic, environmental, demographic, vascular, neuroendocrine, and other factors. Genetic factors account for about 30% of the familial aggregation of HTN [8]. Therefore, it is important and necessary to identify these factors and their interactions to help control HTN. Researchers pointed out that the small contribution of each genetic factors and the interactions among them make it difficult to identify genetic markers for this disease [9, 10]. Many candidate genes like angiotensin-converting enzyme (ACE), angiotensin-converting enzyme 2 (ACE2), and urotensin 2 (UTS2), have been implicated in EH susceptibility [11, 12]. Furthermore, EH has been associated with a complex relationship of multiple polymorphisms in different genes.
There are several genetic determinants implicated in the pathogenesis of EH. The renin angiotensin aldosterone system (RAAS) is one of the most important pathways in the management and pathogenesis of EH [8]. A number of studies have focused on genetic variation in RAAS genes, especially the ACE2 gene [3, 5, 9, 12]. RAAS plays an important role in the regulation of blood pressure (BP) and electrolyte balance. ACE2 is one of the key components in the RAAS that shares 42% identity with the catalytic domain of somatic ACE. It is a carboxypeptidase that plays a protective role in the regulation of BP homeostasis and cardiac function [3, 13]. The ACE2 enzyme is encoded by a 40-kb ACE2 gene, which has been mapped to Xp22. The ACE2 gene contains 20 introns and 18 exons, which encode a polypeptide of 805 amino acids [14]. In the RAAS pathway, the ACE2 enzyme converts vasoactive angiotensin I (Ang I) to angiotensin 1-9 and angiotensin II (Ang II) to angiotensin 1-7 (Ang 1-7) [15, 16]. This enzyme is an important modulator of the clinical manifestations of HTN, cardiovascular diseases (CVD) and kidney abnormalities by converting Ang II into Ang 1-7. The resulting Ang 1-7 causes diuresis, natriuresis, and systemic and localized vasodilation [17].
Polymorphisms in RAAS components are an attractive focus of genetic research on hypertension due to their significant role in regulating BP and individual susceptibility to the condition. The ACE2 gene exhibited multiple allelic variations, including rs2285666, rs1514283, rs4646155, rs4646176, and rs879922 as reported in previous studies [5, 18]. Among these variants, rs2285666 (G > A, intron 3/4), also known as G8790A, is the extensively studied single-nucleotide polymorphism (SNP) of the ACE2 gene in different ethnic populations with HTN [2, 19, 20, 21]. This A allele is associated with greater ACE2 levels in the blood serum of healthy individuals, diabetic subjects, and cerebral stroke patients [22].
The SNP G8790A of ACE2 has been reported to be correlated with HTN, cerebral stroke, coronary heart disease and diabetes [23]. Besides, Pan et al. [2] concluded that the ACE2 G8790A polymorphism is not only associated with EH but also shows geographical, ethnic, and gender diversity. The association between the ACE2 G8790A polymorphism and HTN remains controversial across ethnic groups, as numerous studies have failed to establish a significant link [18, 24]. However, the correlation of ACE2 SNPs with HTN in the Bangladeshi population is not yet reported.
The aim of the study. This research sought to investigate the association between the ACE2 gene polymorphism (G8790A), epidemiological factors, and genders (male and female) with the clinical manifestations of HTN among the population of the southern part of Bangladesh.
Materials and methods
Study design, period and ethics statement
A case-control study was carried out from September 2022 to June 2024 at the Department of Genetic Engineering and Biotechnology, University of Chittagong, in collaboration with the Department of Medicine, Chittagong Medical College (CMC), Chattogram, Bangladesh. This study and questionnaire were approved by the Ethical Review Committee of CMC (Memo no: CMC/PG/2022/247), Chattogram, and all methods were conducted in accordance with relevant guidelines and recommendations. For this study, a total of 494 participants were enrolled, and they were divided into two groups: the case group consists of 260 essential hypertensive patients (male = 144, female = 116) attending the medicine ward of CMC, Chattogram, Bangladesh and the control group consists of 234 healthy normotensive individuals (male = 194, female = 40) were collected randomly from different wards of CMC. The inclusion criteria for HTN subjects were: (i) EH diagnosed (SBP ≥140 mmHg/DBP ≥90 mmHg) according to the WHO guideline of HTN [25] and registered at CMC, and (ii) confirmation that all the subjects are of Bangladesh origin. The selected controls were healthy individuals having normal blood pressure (SBP/DBP 120–129/80–84 mmHg) with no other symptoms of HTN.
The exclusion criteria were: (i) presence of any infectious disease, (ii) conditions where phlebotomy is contraindicated, (iii) age less than 18 years and greater than 70 years, (iv) pregnancy and (v) unwillingness to participate in the study. All procedures were designed and executed to ensure full compliance with the ethical clearance and to uphold the principles for research involving human subjects. Before the interview, the participants were briefed on the research purpose, and written informed consent was taken. All participants (n = 494) were interviewed face-to-face with a standardized and pre-tested questionnaire. Socio-demographic and clinical information for each subject was collected and reviewed by a health professional. Moreover, participants' data, including written consent forms, were methodically documented, with confidentiality assured by removing their names and storing them in a secure and restricted place.
Data collection procedure
The structured questionnaire was administered by experienced nurses to collect demographic and epidemiological data. The general characteristics (e.g., age and its category, body mass index, blood pressure, gender, dwelling place, education), behavioral characteristics (such as smoking/tobacco consumption, consumption of fruit, vegetable, meat, physical activity and additional salt intake) were obtained through interviewing both HTN patients and controls with the questionnaire. The body mass index (BMI; kg/m2) of the participants was measured using calibrated equipment and a standardized protocol. Blood pressure (BP) was measured after a minimum rest period of 30 min in individuals who had consumed hot beverages like coffee. The measurements were taken using a sphygmomanometer at the midpoint of the left arm, with the participant seated and supported by an armrest. BP was measured twice at 5-min intervals, and the average of the two readings was considered the accurate value. The thresholds for elevated BP were set at SBP≥ 140 mmHg and DBP≥ 90 mmHg. Unless otherwise stated, age, BMI and BP were expressed as mean ± SD, and other general and behavioral characteristics were expressed in percentage (%) for all HTN patients and healthy controls.
Collection and processing of samples
From each case and control subject, 5 mL of venous blood samples were obtained using sterilized disposable hypodermic needles. For genomic DNA extraction, a 2 mL fraction of the blood sample was transferred to an EDTA tube (5 mL). The remaining 3 mL sample was taken into another tube and centrifuged at 4000 rpm for 10 min to obtain blood serum. The collected whole blood and serum samples were stored at –20 °C for molecular and biochemical analyses. Urine samples were also collected in sterile urine vials and preserved carefully until analysis.
Genomic DNA extraction, PCR amplification and RFLP
The rs2285666 polymorphism of the ACE2 gene was initially detected by polymerase chain reaction (PCR)-restriction fragment length polymorphism (RFLP) analysis of genomic DNA (gDNA). The gDNA was extracted from peripheral whole blood of both HTN patients and controls utilizing the commercial ReliaPrep™ Blood gDNA Miniprep System (Promega, USA) according to the manufacturer’s instructions. During gDNA isolation, proteinase K (20 µL) was added to the reaction mixture to inhibit protease activity if it occurred in the sample or reaction mixture. The primers were designed to amplify a unique region specifically from 19803 bp to 20268 bp within the 40 Kb ACE2 gene sequence. The gDNA was amplified through PCR by targeting the region carrying the G8790A SNP of the ACE2 gene with forward and reverse primer pairs [21]. The amplification was conducted in a final volume of 15 μL containing 7.5 μL master mix (New England Biolabs Inc., USA), 1 μL template gDNA, 1 μL (10 μM) of each primer, and 4.5 μL nuclease-free water. To amplify the targeted ACE2 polymorphism (rs2285666), a 32-cycle PCR profile was performed at optimal conditions using a thermal cycler (Nyx Technik Inc., USA), which included initial denaturation at 94 °C for 5 min, denaturation at 94 °C for 30 s, primer annealing at 58 °C for 40 s and elongation at 72 °C for 40 s. The final extension lasted for 5 min at 72 °C. The resulting PCR product was digested with the restriction enzyme AluI (New England Biolabs Inc., USA) at 37 °C for 3 h. At the end of incubation, the enzymatic reaction mixture was heated to 80 °C for 20 min to stop the digestion. The target fragments of the ACE2 gene were screened by agarose gel (2%, w/v) electrophoresis and were visualized under a UV transilluminator (Benda, Germany). The PCR product of the rs2285666 allele of the ACE2 gene was stored at –20 °C until analysis.
Genotyping of ACE2 polymorphism
The genotyping of the ACE2 gene polymorphism rs2285666 (G>A) was carried out using the PCR-RFLP, followed by confirmation through gene sequencing. During PCR, primer pairs were designed to bind within intron 3 of the ACE2 gene, with the forward primer annealing at positions 19,803-19,823 bp and the reverse primer at positions 20,249-20,268 bp. The ACE2 gene is located on the Xp22 region of the X chromosome and consists of 20 introns and 18 exons. Amplification produced a single fragment of 466 bp, which was visualized by electrophoresis on a 1.5% (w/v) agarose gel using a 100 bp DNA ladder as a reference. To assess the rs2285666 polymorphism, the PCR amplicons were digested with the restriction enzyme AluI. This digestion generated distinct banding patterns corresponding to the different genotypes: a single undigested fragment of 466 bp for the wild-type GG genotype, two fragments of 281 bp and 185 bp for the homozygous AA mutant genotype, and three fragments of 466, 281, and 185 bp for the heterozygous AG genotype.
Sequencing of the PCR amplicon
To confirm genotyping of the ACE2 gene polymorphism rs2285666, 10% of the total cases and controls were randomly selected for re-amplification by PCR. The obtained PCR amplicons were sequenced by a genetic analyzer (ABI PRISM 3100, Applied Biosystems, USA). All segments were sequenced in both directions to ensure any nucleotide differences. Sequence variations were examined using DNA-based tools [26] and the Clustal Omega alignment tool [27].
Clinical and biochemical parameters
The blood serum samples were analyzed with an autoanalyser (Dimension, Siemens, Germany) to determine the following biochemical parameters: total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, and serum creatinine. Urine samples were tested immediately to determine the qualitative albumin level in both hypertensive and control subjects.
Data processing and analysis
The confirmation of Hardy-Weinberg equilibrium (HWE) was achieved through the chi-square (χ2) test. All statistical analyses were conducted using R Studio (V.4.3.1). The comparison of genotype and allele distributions between the HTN and control groups was assessed using chi-square tests. A rigorous test estimating 2 values at the 0.05% level of significance was performed to determine whether the genotypic frequencies of the ACE2 polymorphism departed from HWE. Variables that did not meet the standard limit were excluded from the analysis. The odds ratio (OR) with a 95% confidence interval (CI) was used to evaluate the relationship between genotype and HTN. Relative risk (RR) estimation (95% CI) was applied to confirm the likelihood of disease incidence for different genotypes. Genotype and allelic frequencies in case and control groups were tested using logistic regression before and after adjustment for categorical variables. The results were considered statistically significant if the P-value was < 0.05.
Results
Analysis of general characteristics
The general characteristics were employed to collect sociodemographic and epidemiological variables. These variables are assessed extensively in HTN studies to understand risk factors, identify health disparities and design targeted interventions for different ethnic populations [3, 28]. Moreover, these factors help to highlight the racial disparities in terms of HTN outcomes. This study evaluated ten sociodemographic variables, such as gender, age, age category, BMI, SBP, DBP, residential area, educational status, occupation, and family history of HTN to examine the epidemiological differences between the HTN case and control groups. Table 1 presents the general characteristics, including sociodemographic variables, of study participants. The mean age of the case and control groups was 45 ± 9 and 39 ± 8, respectively.
The higher average age was observed among HTN cases, which may be attributed to the increased risk of developing HTN with older age. Categorizing the age, the 40-49 year group had the highest number of hypertension cases (44%), while the 25-39 year group had the maximum (62%) healthy controls (Table 1). The BMI value of the case was slightly higher (23.65 ± 3.65 kg/m2) than that of the control (22.37 ± 1.62 kg/m2). This result suggested that individuals in the case group have a higher prevalence of high body weight compared to the control group. The average SBP of the case and control groups was 142 ± 2 and 120 ± 2 mmHg, with the corresponding DBP being 86 ± 12 and 80 ± 3 mmHg, respectively. The higher SBP value of the case group indicated a greater prevalence of HTN among the studied populations. According to the study, 58% of patients with hypertension lived in rural areas, compared to 69% of healthy subjects who lived in urban areas.
The higher proportion of patients from rural areas suggested a lower level of awareness about HTN. Only 11% of patients had a bachelor's or higher degree and 46% of patients with primary education, whereas 59% of healthy participants had a bachelor's or higher degree (Table 1). The higher percentage of educated individuals in the control group may suggest better health literacy and healthier lifestyle choices, potentially contributing to their lower HTN prevalence. In case of occupation, 38% of the cases were housewives and 74% of the controls were in service. However, there was no significant statistical difference (P = 0.6) between the cases and controls regarding the family history of HTN.
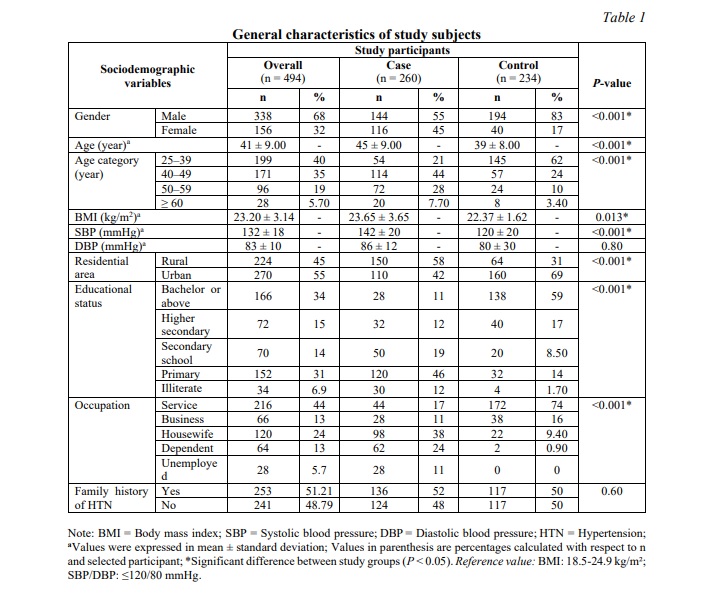
The aforementioned results highlighted the statistically significant socio-demographic differences (P <0.001) between case and control groups in terms of general characteristics, including gender, age, age category, BMI, SBP, residential area, education, and occupation. The other two variables, such as DBP and family history of HTN, showed insignificant differences (Table 1) in the study.
Analysis of behavioral characteristics
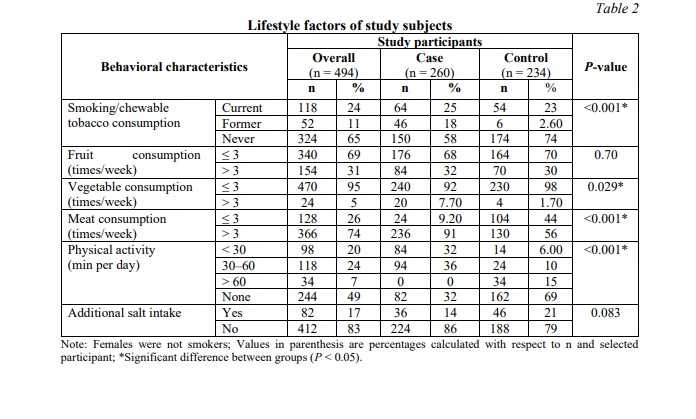
The lifestyle factors as well as behavioral characteristics are crucial in the development, progression, and management of HTN [29]. Thus, it is necessary to study these factors for designing effective strategies in order to prevent and treat HTN by comprehending their impact on the conditions. In this study, six lifestyle variables, including smoking/tobacco consumption, frequency of consuming fruits, vegetables, and meat, physical activity, and additional salt intake, were examined to determine the behavioral and/or dietary habit differences between the case and control groups. The lifestyle features of the study participants are summarized in Table 2. Individuals with HTN have a higher proportion of current (25%) and former (18%) smokers compared to the healthy controls (P < 0.001). There were no significant differences (P = 0.7) observed in fruit consumption frequency between the cases and controls.
The practice of vegetable and meat consumption (times per week) was found to be significantly higher in controls, which implied the importance of healthy and balanced food intake for preventing HTN. Moreover, the control group had a higher proportion of people engaged in more daily physical activity (P < 0.001) than HTN subjects (Table 2), which might play an important role in avoiding HTN complications. The percentage of additional salt intake did not show a significant difference (P = 0.083) between the study groups. The significant differences were observed between the case and control groups concerning smoking/tobacco consumption, vegetable and meat intake, and physical activity level. There were no significant differences between the groups in terms of fruit consumption or additional salt intake.
Genotyping results of the ACE2 polymorphism
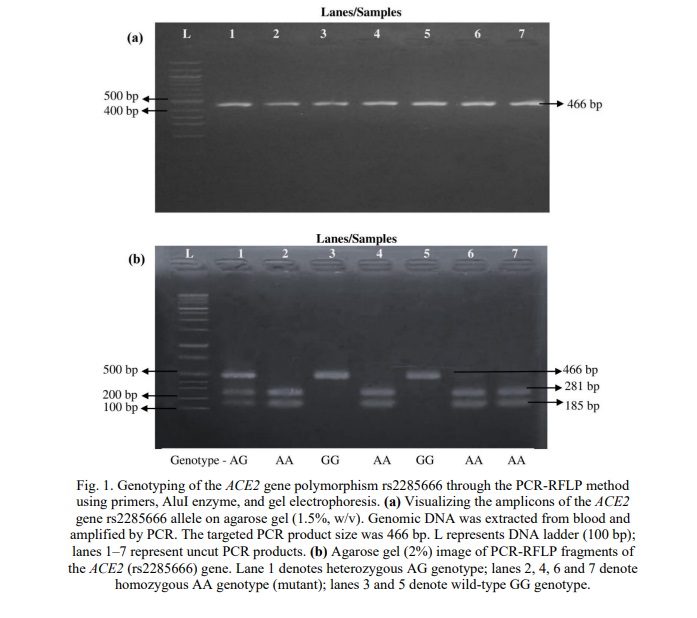
The banding patterns of PCR products and its restriction fragments for the rs2285666 polymorphism in the ACE2 gene are illustrated in Fig. 1. The uncut PCR products showed a single amplicon of 466 bp in all samples, confirming the successful amplification of the rs2285666 region of the ACE2 gene (Fig. 1a). After digestion with the AluI enzyme, distinct banding patterns corresponding to different genotypes were observed. A single band of 466 bp was detected in lanes 3 and 5, indicating the homozygous wild-type GG genotype. Two bands of 281 bp and 185 bp were observed in lanes 2, 4, 6, and 7, representing the homozygous mutant AA genotype. Three bands of 466 bp, 281 bp, and 185 bp were present in lane 1, corresponding to the heterozygous AG genotype (Fig. 1b). These banding patterns confirmed the occurrence of genetic variation at the rs2285666 locus of the ACE2 gene. Furthermore, the distribution of the genotypes in the studied population showed no significant deviation from Hardy-Weinberg equilibrium (HWE).
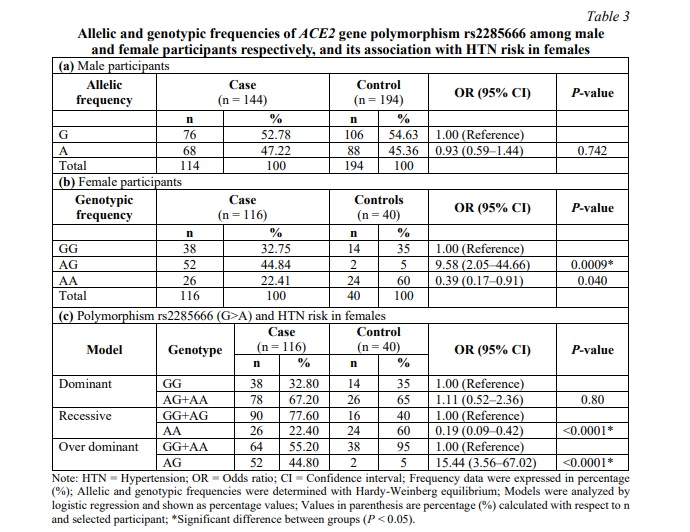
The allelic and genotypic frequencies of the rs2285666 allele of the ACE2 gene were investigated using HWE among males and females, respectively. The association between the rs2285666 (G>A) and the risk of EH in female participants was also explored in this study. Table 3 represents the frequencies of the ACE2 gene polymorphism rs2285666 (G>A) in male and female subjects and its association with EH risk, specifically in females. The G allele frequency was observed in 52.78% of male HTN cases and 54.63% of male controls, while the A allele was found in 47.22% of male HTN cases and 45.36% of male controls (Table 3a). In males, no significant difference was observed between the A and G alleles. Since ACE2 is an X-linked gene and males carry only one copy of the X chromosome, genotypic distribution was not applicable due to the absence of allelic variation. In females, the AG genotype was significantly associated with the higher risk of HTN, occurring in 44.84% of cases and 5% of controls (P = 0.0009). Moreover, the AA genotype was found to be about 3.99 times less likely to be a risk factor for HTN in females when compared with the GG genotype (Table 3b).
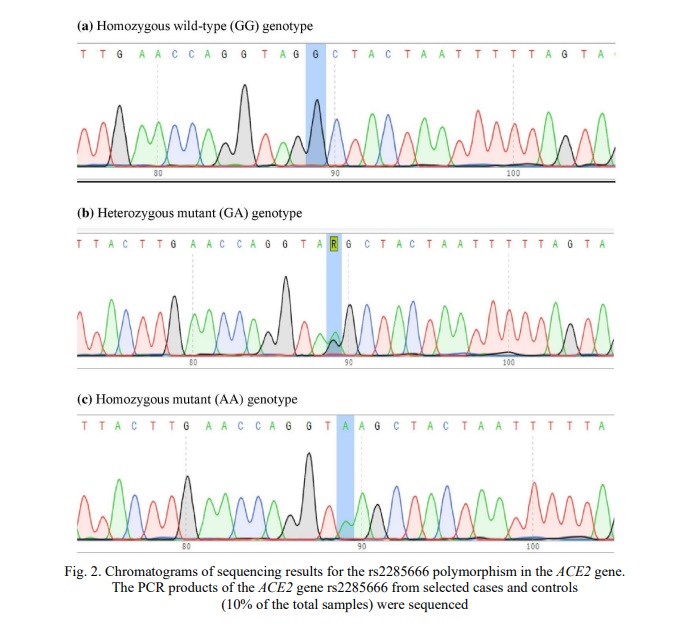
The PCR products of rs2285666 from randomly selected cases and controls were sequenced to validate the genotyping method. The chromatograms of sequencing results for the rs2285666 polymorphism in the ACE2 gene are depicted in Fig. 2. In chromatograms, the nucleotides are color-coded as red, green, blue and black for thymine (T), adenine (A), cytosine (C), and guanine (G) respectively, to clearly distinguish each base in DNA sequences. In Fig. 2a, the G allele was present in two copies in the study people as indicated by the chromatogram with peaks predominantly in blue. This result reflected that the genotype was homozygous for the G allele (GG). The chromatogram with blue and green curves represented a heterozygous genotype as GA (Fig. 2b). These findings suggested that the individuals with this genotype have one mutant (A) allele and one wild-type (G) allele at the rs2285666 locus. A consistent green curve demonstrated the homozygous mutant (AA) genotype with peaks predominantly in green. It indicated that the rs2285666 locus has two identical mutant (A) alleles (Fig. 2c). This genotype resulted in two copies of the A allele in an individual. Therefore, it is mentioned that the AG genotype of the rs2285666 allele in females was significantly linked to the higher risk of HTN (44.8% cases vs. 5% controls), while the AA genotype showed no significant association (22.4% cases vs. 60% controls).
Association of the ACE2 gene polymorphism with HTN risks
A multivariate logistic regression analysis was conducted to estimate the relationship between the ACE2 gene polymorphism rs2285666 (G>A) and HTN risk in female participants. The Odds ratios (OR) with 95% confidence interval (CI) were calculated to quantify this association for both case and control groups. This analysis was performed only in female subjects as the ACE2 gene is located on the X chromosome. According to the dominant model (Table 3c), which compares GG to the combined AG+AA genotypes, there was no significant association with HTN risk in females (P = 0.08). In the recessive model, the AA genotype was more frequent among controls than cases, indicating a protective effect against HTN. In contrast, under the dominant model, the AG genotype appeared more frequently in hypertensive patients than in controls, suggesting an increased risk of HTN (Table 3c). These findings consistently showed that the AG genotype was associated with a higher risk of HTN in females across different models, whereas the AA genotype was related to a reduced risk. The association of the rs4646994 allele with HTN was examined through frequency distribution (Table 3a), with interpretation adjusted for the fact that males carry only one copy of the X-linked gene.
Analysis of clinical and biochemical parameters
This study examined the clinical and biochemical profiles of male and female participants, with a focus on comparing case and control groups, to identify significant gender differences in various health parameters. The clinical and biochemical characteristics, including SBP, DBP, TC, TG, HDL, LDL, serum creatinine, and urine albumin, are listed in Table 4.
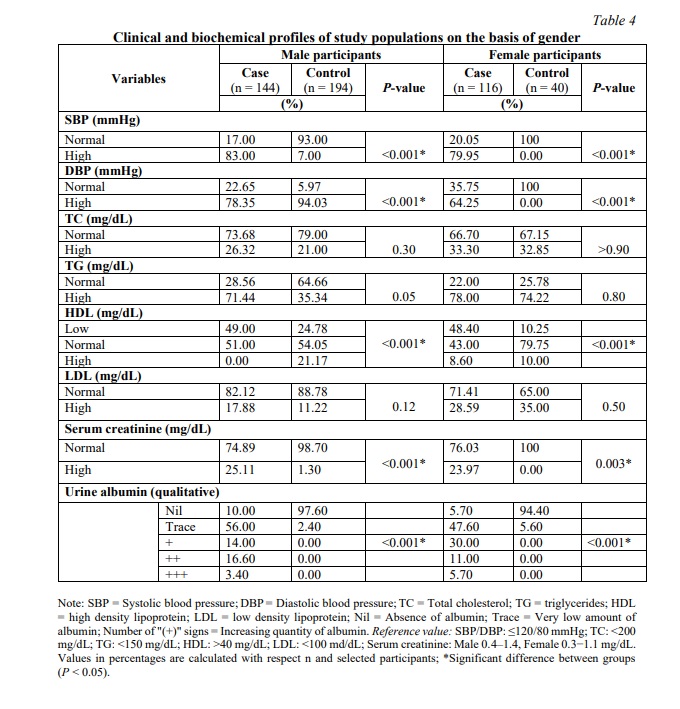
Among male participants, 83% of cases exhibited high SBP compared to 7% of controls, showing a significant difference (P < 0.001). Similarly, 78.35% of cases had high DBP compared to 94.03% of controls, which was also statistically significant (P < 0.001). Regarding lipid profiles, TC levels did not show a significant difference between cases and controls (P = 0.30), with 26.32% of cases and 21% of controls having high TC levels. However, TG levels were considerably elevated in cases, with 71.44% having high TG values compared to 35.34% of controls, approaching statistical significance (P = 0.05) (Table 4). The higher TG values indicated the potential role of dyslipidemia in the progression of HTN.
The HDL cholesterol levels revealed a significant distinction, with 49% of cases having low HDL compared to 24.78% of controls (P < 0.001) in males. Conversely, 21.17% of controls had high HDL values, while none of the cases had higher HDL levels. The low level of HDL in HTN patients was probably due to the HTN-related metabolic complications. For male participants, 17.88% of HTN cases had high LDL cholesterol levels compared to 11.22% of controls, with no significant difference (P = 0.12). Serum creatinine levels were significantly higher in the case group, with 25.11% having elevated levels compared to 1.30% of controls (P < 0.001). The quantitative levels of urine albumin differed significantly, with 97.60% of controls having no albumin compared to only 10% of cases, while higher albumin levels (+, ++, +++) were observed exclusively in cases (P < 0.001).
For female participants, the SBP showed a significant difference between cases and controls (P < 0.001), with 79.95% of cases having high SBP compared to none of the controls (Table 4). The DBP levels also showed a significant disparity (P < 0.001), with 64.25% of cases having high DBP, whereas all controls had normal DBP. The TC values among females did not show significant differences between cases and controls (P > 0.9), with 33.30% of cases and 32.85% of controls having high TC. Similarly, TG levels did not differ significantly (P = 0.80), with 78% of cases and 74.22% of controls having high TG. However, HDL cholesterol levels presented a significant difference (P < 0.001); 48.40% of cases had low HDL compared to 10.25% of controls. LDL cholesterol levels did not show significant differences (P = 0.5), with 28.59% of cases and 35% of controls having high LDL levels. Serum creatinine levels were significantly higher in the case group (P = 0.003), with 23.97% of cases having their elevated levels compared to none of the controls. Urine albumin levels also showed significant differences (P < 0.001), with 94.40% of controls having no albumin compared to only 5.70% of cases, while higher albumin levels were more prevalent in cases (Table 4). The biochemical analyses demonstrated that the high levels of serum creatinine and urine albumin in male and female HTN patients could be attributed to impaired kidney function associated with EH.
Table 5 presents the influence of the ACE2 G8790A polymorphism on clinical and biochemical profiles in male and female HTN patients. In male hypertensive patients, the ACE2 G8790A polymorphism showed no notable association with BMI, blood pressure, TC, TG, LDL, serum creatinine and urine albumin level, although reduced HDL levels were more frequent in G allele carriers. In female hypertensive patients, the distribution of BMI and SBP did not differ notably across genotypes. However, DBP was higher in AG and GG carriers compared to AA. TC and TG were also elevated among AG and GG groups. Significant variation was observed in serum creatinine levels (P = 0.012), with AA carriers more often within the normal range (Table 5). Urine albumin excretion differed significantly across all three genotypes, with the highest (+++) amount observed in female AA carriers (P = 0.001).
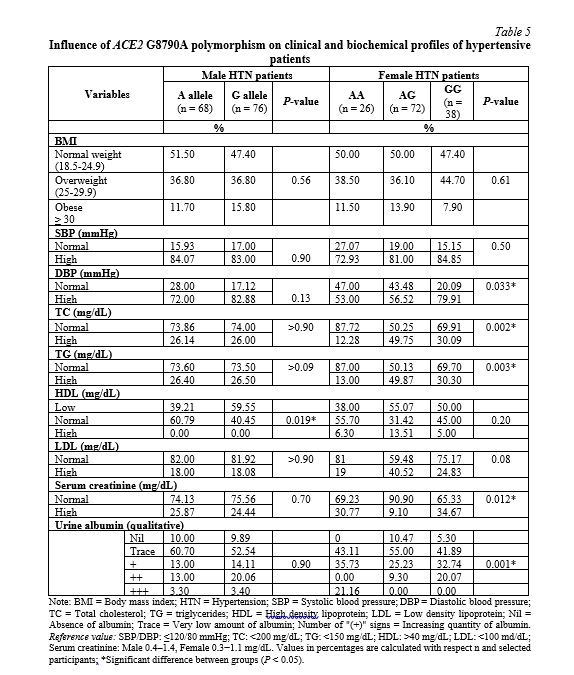
For female HTN patients, SBP levels were high across all genotypes with no significant differences (P = 0.5). DBP was significantly higher in GG genotype carriers (79.91%) compared to AA (53%) and AG (56.52%, P = 0.033). The levels of TC were significantly higher in AG carriers (49.75%) compared to AA (12.28%) and GG (30.09%, P = 0.002). The TG levels also showed higher values in AG (49.87%) carriers compared to AA (13.00%) and GG (30.30%) genotype carriers (Table 5). The HDL cholesterol levels did not show significant differences (P = 0.20). The LDL cholesterol levels approached significance (P = 0.085), with AG carriers having higher levels. Serum creatinine was significantly higher in GG carriers (34.67%) compared to AA (30.77%) and AG (9.10%, P = 0.012). The levels of urine albumin differed significantly (P = 0.001), with higher levels in AA and GG carriers. It is highlighted that the ACE2 G8790A polymorphism significantly affected the specific biochemical factors such as TC, HDL, LDL, serum creatinine, and urine albumin in male and female HTN patients. Males with the G allele had lower HDL levels, while no other parameters showed significant differences on the basis of allele. However, females with the AG genotype had higher TC and lower serum creatinine levels, and GG carriers had higher DBP and urine albumin levels.
Association of ACE2 Genotypes with Physical Activity and Smoking Status
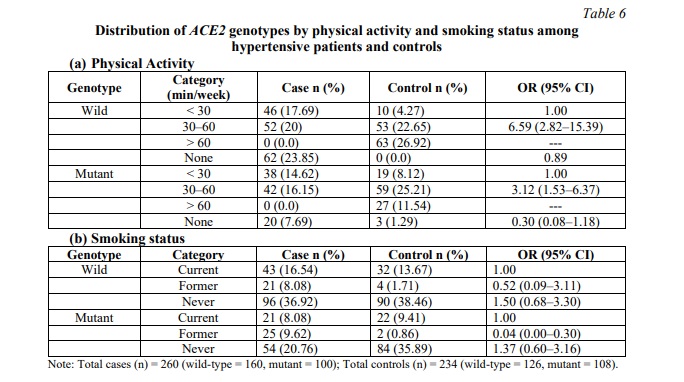
Table 6 shows the distribution of ACE2 genotypes by physical activity and smoking status. Among individuals with low physical activity (<30 min/week), wild-type participants had a higher number of cases compared to controls, while moderate activity (30-60 min/week) was associated with the largest number of cases for both wild-type and mutant genotypes (Table 6a). For physical activity above 60 min, all participants were controls, regardless of genotype. As shown in Table 6b, former smokers with the mutant genotype had very few cases, whereas never smokers with the wild-type had more cases. This suggests differences in risk patterns across genotype groups.
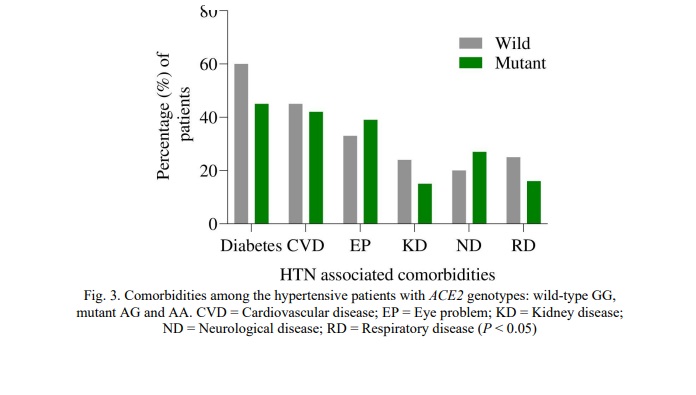
Comorbidities in HTN patients
Different genotypes (wild-type GG and mutant AG, AA) of the ACE2 gene polymorphism rs2285666 (G8790A) were studied to evaluate their impact on various comorbidities among HTN individuals. The distribution of comorbidities in HTN patients revealed significant differences among the wild-type GG, mutant AG, and AA genotypes. The comorbidities in HTN patients with different ACE2 genotypes are shown in Fig. 3. Among the comorbidities, diabetes was more frequently observed in patients with the GG genotype, though this association was marginally significant (P = 0.049). Cardiovascular disease (CVD) showed the highest prevalence in both wild-type GG and mutant AG, AA genotypes without statistically significant (P > 0.05) difference (Fig. 3). There were no significant differences between the wild and mutant genotypes for other comorbidities such as eye problems (EP), kidney disease (KD), neurological disease (ND) and respiratory disease (RD). This study revealed that HTN patients with distinct genotypes of the ACE2 gene displayed diverse comorbidity profiles, with mutant genotypes (AG and AA) commonly associated with a higher prevalence and severity of diabetes and CVD, as well as increased risks of EP, ND, RD, and KD conditions.
Discussion. Essential hypertension (EH) is one of the most common and serious public health problems, and is responsible for high cardiovascular morbidity and mortality worldwide [11]. In Bangladesh, several factors such as rapid urbanization, sedentary lifestyles, poor eating habits, increased cigarette use, and rising CVD rates may contribute to HTN [30]. Numerous genes and non-modifiable factors contribute to BP regulation in a polygenic manner [31]. This study identified notable sociodemographic and behavioral disparities between the HTN patients and healthy controls. The percentage of male HTN patients was significantly higher than that of females, which is consistent with previous studies [32, 33]. Age was identified as a significant risk factor, with HTN patients having a higher mean age than controls, aligning with prior research [34]. The highest HTN prevalence was observed in the 40-49 year age group, contrasting with an earlier study that showed the 50-59 year age group as the most prominent risk group [28]. The HTN patients had higher BMI, SBP, and DBP (Table 1). Besides, they resided in rural areas, had lower levels of education, higher smoking rates, and lower levels of physical activity, with fewer reporting regular exercise and vegetable intake [3, 28]. These findings highlight the need for targeted interventions to address HTN disparities and improve public health.
The effect of the ACE2 gene polymorphisms on HTN is controversial across distinct ethnic populations [9, 18, 34, 35]. Hence, this study investigated the association between the ACE2 gene polymorphism rs2285666 and HTN in southern Bangladeshi populations. No allele frequency difference was found in males (Table 3a), which is comparable with a meta-analysis [18] for the HTN case and control groups. In the current study, different genetic models of inheritance were utilized to assess the correlation between the ACE2 G8790A gene polymorphism and HTN risk in females solely, as this gene exists on the X chromosome. In the dominant model, no significant relationship was found for AG+AA/GG frequency (Table 3c). The recessive model showed that the AA genotype may exert a protective effect against HTN in females, as it was more prevalent in the control group than in the case group. It indicated a significant inverse relationship between the AA genotype and HTN risk in females (Table 3c). In accordance with these findings, Li [18] explored the ACE2 gene polymorphism in women using dominant and recessive models, and the author reported that both models demonstrated an insignificant association between the ACE2 G8790A polymorphism and HTN risk.
Additionally, no significant differences in genotypic distribution were observed between female cases and controls in this study. A previous research also reported no significant variation in genotype frequencies [34], consistent with the obtained results for the AA and AG genotypes, although their data differed slightly for the AG genotype. In contrast to these reported findings, this research revealed that females with a heterozygous AG genotype were at an increased risk of developing hypertension compared to those with a GG genotype (Table 3b). This result is further supported by the dominant model (Table 3c), which highlighted a markedly increased risk of HTN among females carrying the AG genotype compared to other genotypes. In a community-based study conducted in central China, the authors [35] reported that analysis of a single SNP (rs2285666) showed no significant differences in minor allele frequency (A) among females in dominant, recessive, and additive models, nor were any differences observed among male patients. Contrasting findings were reported, with significant genotype and allele frequency differences in HTN patients in the Dongxiang population compared to controls, including a higher prevalence of the AA genotype and the A allele, regardless of gender. Furthermore, Dongxiang HTN patients showed higher AG and AA genotype frequencies and a higher A allele prevalence than Han HTN patients [12].
Several studies have reported a positive association between G8790A and HTN [9, 36]. Therefore, the function of the ACE2 G8790A SNP in HTN remains a subject of debate due to conflicting findings. Such heterogeneous findings regarding the relationship between the rs2285666 gene polymorphism and HTN can be attributed to the following factors. Firstly, hormonal factors and differences in sex chromosomes play a vital role in BP variations between males and females [12, 19, 37]. Secondly, genetic factors, including significant variations in the frequency of ACE2 variants, exist across racial and ethnic groups, further contributing to this heterogeneity [12, 38]. The present study found no association between the G8790A allele (A) and HTN in male patients, consistent with several previous studies, although it revealed a new finding, a significantly higher frequency of the heterozygous mutation (AG) in female HTN patients (Table 3a, b).
A previous study on the association between the G8790A polymorphism and type 2 diabetes mellitus reported a higher frequency of the heterozygous (AG) mutation in females [39], but no other studies have reported this association in female patients. This novel finding was detected probably due to the interaction between A and G alleles in the heterozygous state, which influences gene expression or regulatory mechanisms differently in females, potentially contributing to HTN risk, while the allelic interaction might not be prominent in males. Additionally, rs2285666 exhibits properties of a quantitative trait locus for HTN, a DNA region linked to a distinct phenotypic trait that varies in degree and is known to show a polygenic effect [40]. It is plausible that HTN is influenced by multiple genes and environmental factors (including geographic location), rather than being solely determined by a single gene.
The clinical and biochemical profiles were compared between male and female participants in this study. Hypertensive patients showed higher SBP and DBP values, along with lower HDL cholesterol levels (Table 4), consistent with previous findings in a study conducted in Spain [41]. Elevated serum creatinine in both males and females indicated possible renal impairment, in agreement with earlier research [42]. Urine albumin levels were significantly higher in cases, as supported by numerous studies [43, 44]. By contrast, TC, TG and LDL did not show notable differences between cases and controls in either gender.
The ACE2 gene polymorphism rs2285666 was studied to evaluate its impact on the biochemical variables in male and female HTN patients (Table 5). In males, differences in HDL cholesterol levels suggested that allele variation may influence lipid metabolism, although no consistent effects were observed for other clinical variables. In female HTN patients, GG genotype carriers had higher DBP and serum creatinine levels, AG carriers showed elevated TC levels, and AA carriers had higher urine albumin levels. Thus, no consistent risk genotype for biochemical parameters was identified, highlighting the need for further studies with larger sample sizes. Pinheiro et al. [9] reported no statistically significant impact of the G8790A variant on clinical factors in HTN patients of both genders. Table 6 demonstrates that ACE2 genotypes may influence the relationship between physical activity, smoking status, and HTN risk. Differences in case distributions across activity levels and smoking categories suggest a potential gene-environment interaction, but further data are needed to confirm these associations.
The impact of the ACE2 rs2285666 genotypes (GG, AG, and AA), on various comorbidities in HTN patients was assessed (Fig. 3). The GG genotype was marginally linked to a higher frequency of diabetes, while CVD was prevalent across all genotypes. Yang et al. [36] similarly reported that the G8790A variant might increase myocardial infarction (MI) risk in females and, when combined with alcohol consumption, raise the likelihood of chronic heart disease and MI risk in males. No clear genotype-related differences were observed for other comorbidities, including EP, KD, ND and RD. Mutant genotypes (AG, AA) were connected to higher prevalence and severity of diabetes, CVD, and other health conditions. This study identified a novel association between the ACE2 G8790A polymorphism and increased HTN risk in females with the AG genotype. It underscores the importance of genetic and gender differences in HTN management. However, the small sample size and focus on southern Bangladeshi populations limit generalizability. Further research with larger samples is needed.
Conclusion. HTN is a multifactorial and polygenic condition affecting about one-third of the global population and is progressively becoming a serious health issue in Bangladesh. The impact of the ACE2 gene polymorphism on essential hypertension was investigated to identify sociodemographic and genetic factors associated with HTN in the southern region of Bangladesh. The research pointed out the risk-associated polymorphisms in HTN patients using the PCR-RFLP method with ACE2 G8790A-specific primers and the AluI enzyme to detect the specific SNP. This study revealed that the heterozygous AG genotype of the ACE2 gene is associated with an increased risk of HTN, suggesting its potential as a biomarker for early diagnosis and the prevention of complications. The ACE2 gene polymorphism significantly affected the serum creatinine, urine albumin, TC, HDL, LDL in male and female HTN patients, which can lead to kidney disease and cardiovascular disease (CVD). HTN patients with different ACE2 gene genotypes indicated the varied comorbidities with mutant genotypes (AG and AA) usually linked to a higher prevalence and severity of diabetes and CVD conditions. Additionally, environmental factors such as diet and lifestyle might play a significant role in HTN prevalence. This work underscores the importance of considering both genetic and environmental factors in developing public health strategies to challenge the growing burden of HTN. By highlighting the interplay among these factors, this study will contribute to a deeper understanding of HTN in the Bangladeshi population and offer valuable insights for more effective, and targeted healthcare interventions in future research and public health management. Understanding the impact of the ACE2 gene polymorphism on hypertension will not only help in tailoring more personalized treatment approaches for HTN patients but also address their specific comorbidities more effectively.
Financial support
This study was funded and supported by the Grants for Advanced Research in Education (GARE) program under the Ministry of Education, Government of the People’s Republic of Bangladesh (PID: LS20222237; GO No: 37.20.0000.004.033.020.2022-596) and the Research & Publication Cell (RPC: 503/2023–24/2nd Call/33/2024), University of Chittagong.
Conflict of interests
The authors have no conflict of interest to declare.
Thanks
The authors thank the Next-generation Sequencing, Research and Innovation Laboratory Chattogram (NRICh), Disease Biology and Molecular Epidemiology (dBme) Research Group, Department of Genetic Engineering and Biotechnology, University of Chittagong; Department of Medicine, Chittagong Medical College, Chattogram, Bangladesh, for their constant support throughout the study. The authors also thank the patients enrolled in this research for making this work possible. The research team gratefully acknowledges the Asperia Healthcare Ltd., Chattogram, for providing biochemistry lab facilities. The authors acknowledge the Grants for Advanced Research in Education (GARE) program, and the Research and Publication Cell, University of Chittagong, Bangladesh, for financial assistance














Reference lists