
Optimization of Naltrexone and Nicotine Co-Delivery via PVP/PVA Microneedle Systems: A Translational Approach
Abstract
Background: Addiction to alcohol and nicotine remains a global health challenge, with current treatment options often hindered by issues of frequent dosing and low patient adherence. Transdermal drug delivery systems, such as microneedle patches, offer a promising solution to overcome these limitations by enabling controlled and sustained drug release. The aim of the study:To optimize and characterize microneedle patches for the transdermal delivery of Naltrexone HCl and Nicotine USP to support alcohol and smoking cessation. The goal is to enhance treatment efficacy and patient adherence through advanced drug delivery systems. Materials and methods: The research began with preformulation analyses to assess the solubility, thermal behaviour, and structural integrity of the drugs, ensuring their suitability for incorporation into microneedle patches. Various formulations were developed, varying the concentrations of Polyvinylpyrrolidone (PVP) and incorporating 3% Tween 80 as a permeation enhancer. In vitro studies were conducted to evaluate drug release profiles and permeation capabilities. Results: Microneedle patches demonstrated significant cumulative drug permeation, highlighting their potential for effective transdermal delivery. Formulations with reduced PVP ratios exhibited slower drug release rates. However, the addition of 3% Tween 80 successfully enhanced drug release, achieving complete drug permeation over time. These findings underscore the patches' ability to provide controlled release while maintaining structural integrity. Conclusion: The optimized microneedle patches present a novel approach to managing alcohol and nicotine addiction by addressing challenges related to frequent dosing and adherence. By improving drug delivery efficiency and patient compliance, these systems hold significant potential to enhance the success of addiction treatment strategies
Keywords: Microneedle Patches, Transdermal Drug Delivery, Naltrexone Hydrochloride, Nicotine, Addiction Treatment
Introduction. Addiction, whether to alcohol or nicotine, is influenced by a complex interplay of genetic, environmental, social, and pharmacological factors, though the exact mechanisms remain unclear. Key questions revolve around what factors initiate and sustain substance use and what brain changes lead to compulsive behaviour. Genetic predispositions, including psychiatric disorders such as anxiety and depression, as well as personality traits like impulsivity and antisocial behaviour, play a significant role in increasing the risk of addiction [1]. These predispositions affect neurotransmitter systems and an individual's response to alcohol and nicotine, making them more susceptible to developing an addiction.
Pharmacokinetics also contribute to addiction risk, with genes influencing how substances like alcohol are metabolized [2]. For example, enzymes such as alcohol and aldehyde dehydrogenase affect the way in which alcohol is broken down in the body. Variations in these enzymes can cause aversive reactions to alcohol, potentially deterring further consumption. Acetaldehyde, a byproduct of alcohol metabolism, may mimic some of alcohol's effects and influence neurotransmitter systems, though its precise role is still under investigation. Similarly, nicotine's pharmacokinetics, including its rapid absorption and clearance from the body, play a critical role in the development and maintenance of nicotine dependence. Alcohol exerts its effects by interacting with various receptors and ion channels in the brain, even at low concentrations [3]. It inhibits NMDA receptors, leading to cognitive impairments, and enhances the function of GABAA and glycine receptors, contributing to its sedative effects. Alcohol also modulates serotonin (5-HT3) and neuronal nicotinic acetylcholine receptors (nAChRs), which are involved in reward and reinforcement pathways. These interactions with receptors and ion channels are influenced by their subunit composition, making certain receptors more sensitive to alcohol's effects [4, 5].
Nicotine dependence, which drives tobacco addiction, is similarly complex. Nicotine interacts with nAChRs, which are widely distributed throughout the brain and are involved in the release of various neurotransmitters, including dopamine, noradrenaline, GABA, glutamate, and acetylcholine. These interactions contribute to the reinforcing effects of nicotine, making it highly addictive. Despite the significant health risks associated with smoking, including heart disease, lung disease, and cancer, quitting smoking is challenging, with high relapse rates [6]. About 80% of individuals attempting to quit relapse within the first month, and only about 3% remain smoke-free after six months, highlighting the chronic nature of nicotine addiction [7, 8, 9].
The overlap between alcohol and nicotine addiction extends to the brain's reward pathways, where both substances influence similar neurotransmitter systems. This overlap suggests that addressing both addictions simultaneously might be beneficial, especially considering that nicotine may protect against certain neurotoxic effects of alcohol withdrawal. However, the treatment of dual addiction is complicated by the need to balance interventions that address both substances effectively [10].
Treatment of Smoking in Alcoholics
Individuals with both alcohol and nicotine addiction often face poorer treatment outcomes. Smokers with alcohol dependence are more likely to relapse into alcohol use when they relapse to smoking (Johnson and Jennison, 1992) [11, 12]. They also experience more severe nicotine withdrawal, resulting in lower smoking cessation success rates (Marks et al., 1997; DiFranza and Guerrera, 1990) [13]. Treating these dual addictions remains a major challenge.
Treatment providers have historically been reluctant to address smoking cessation during alcoholism treatment. Smoking was often seen as a lesser concern, or there was a fear that quitting could interfere with alcohol abstinence by increasing stress (Bobo and Gilchrist, 1983) [14, 15]. Additionally, smoking was viewed as a coping mechanism for alcohol cravings and withdrawal, leading providers to avoid disrupting this strategy. Another compelling reason to integrate smoking cessation into alcoholism treatment is the significant health risks associated with smoking among alcoholics, which exceed those related to alcohol alone (Hurt et al., 1996) [16]. Many individuals entering treatment for alcoholism express a willingness to address smoking at the same time, even without formal cessation interventions (Saxon et al., 1997) [17, 18]. Research indicates that successful treatment for alcoholism often coincides with reduced smoking rates and increased motivation to quit (Monti et al., 1995) [17]. Recent studies have also explored pharmacological treatments that could benefit individuals struggling with both alcoholism and smoking, given the overlap in brain reward pathways influenced by these substances. For example, medications like naltrexone and nalmefene, which are effective in treating alcoholism by blocking opioid receptors, also show potential in addressing nicotine dependence (Pomerleau, 1998) [19]. However, their specific efficacy for individuals with both alcohol and nicotine addiction remains under investigation.
The primary objective of this research is to develop and optimize drug delivery systems specifically targeting individuals struggling with both alcohol addiction and smoking habits concurrently. This dual focus is particularly important given that a significant proportion of individuals with alcohol addiction also smoke. Addressing both addictions simultaneously is essential for improving overall treatment outcomes and quality of life for these individuals. To achieve these goals, the study will explore various polymer formulations for swellable microneedle systems, aiming for precise control over the release kinetics of therapeutic agents. Polymers such as polyvinylpyrrolidone (PVP) and polyvinyl alcohol (PVA), will be a focal point to optimize sustained release profiles. These swellable microneedle formulations will provide a minimally invasive method for drug administration, enhancing treatment efficacy and patient adherence through precise control over drug release kinetics. Optimizing the selected polymers' formulations will ensure sustained drug release and reduce the dosing burden, making them particularly beneficial for inaccessible areas of the body.
The aim of the study: To optimize and characterize microneedle patches for the transdermal delivery of Naltrexone HCL and Nicotine USP to support alcohol and smoking cessation. The goal is to enhance treatment efficacy and patient adherence through advanced drug delivery systems.
Materials and methods
Materials
The research utilized several key ingredients, all of which were procured from reputable suppliers. Naltrexone HCl was gifted from Deccan Nutraceuticals Pvt Ltd, while Nicotine USP was gifted from Nico Orgo Marketing Pvt Ltd. Polyvinyl alcohol and PVP K30 were supplied by Molychem Pvt. Ltd. and SD Fine Chem Limited, respectively.
Preformulation Study
Preformulation is a critical step in drug dosage form development, aimed at gathering essential information to create a stable and bioavailable product with minimal drug-excipient interactions and suitable for mass production.
Identification of the Powdered Drug
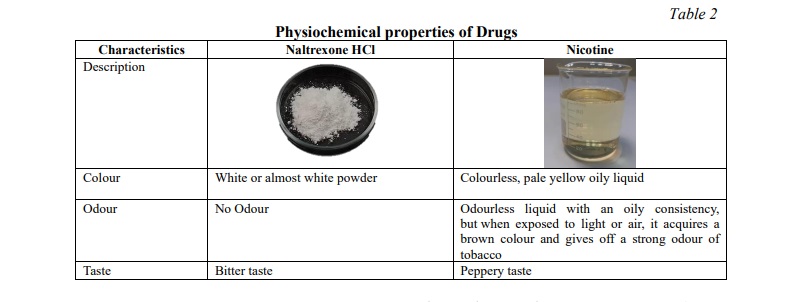
I. Description: Organoleptic properties of the drug, including colour, odour, flavour, and taste, were manually examined.
II. Melting Point Determination: The melting point of Naltrexone HCl was measured using the capillary tube method with a Thiel's tube apparatus. A capillary tube filled with the powdered substance was heated in liquid mineral oil, and the melting point range was recorded and compared to standards [20].
III. IR Spectroscopy: A sample was mixed with KBr, pressed into a pellet, and analysed using FTIR spectroscopy in the 4000-400 cm⁻¹ range. The FT-IR spectrum was compared to reference spectra of Naltrexone HCL and Nicotine to verify drug purity.
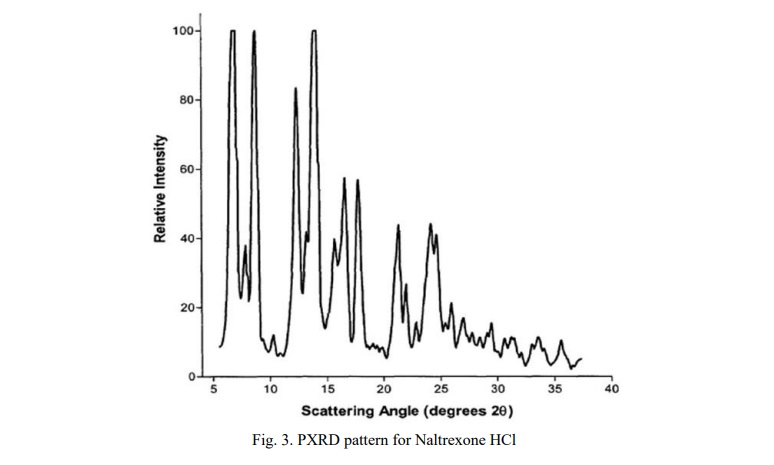
IV. X-ray Diffraction (XRD): PXRD patterns were recorded with a RIGAKU ULTIMA-IV diffractometer using Cu-Kα radiation. Approximately 500 mg of the drug was prepared on a quartz plate, scanned from 5-40° 2θ at a rate of 5° per minute, and compared with standard diffractograms [13].
Physicochemical Tests
Physicochemical tests are crucial for characterizing herbal medicines and ensuring their quality. These tests include:
I. Water Content – Loss on Drying: Approximately 1.5 g of powdered drug was weighed into a tarred porcelain dish. The sample was dried in an oven at 100°C to 105°C until two consecutive weighings showed less than a 0.5 mg difference. After cooling in a desiccator, the final weight was recorded [22].
II. Total Ash Content: About 3.65 g of powdered drug was weighed into a tarred silica crucible. The sample was incinerated in a Muffle furnace with gradually increasing heat until it was free of carbon. The ash was then cooled in a desiccator, weighed, and the percentage of total ash was calculated [23].
Development of Analytical Method and Validation
I. Solubility Test: Solubility of Naltrexone HCl and Nicotine was assessed in various solvents such as ethanol, propylene glycol, glycerine, acetone, and phosphate buffer (pH 7.4). A 5 ml solvent was used, and drug was added in 0.5 g increments to determine the maximum amount that could dissolve.
II. Determination of λmax: λmax was determined by scanning 1000 µg/ml and 100 µg/ml solutions of Naltrexone HCl and Nicotine in selected solvents. For Naltrexone HCl, standard solutions were prepared and diluted in water and phosphate buffer pH 7.4. Absorbance was measured at various concentrations (5-30 µg/ml) using a UV spectrophotometer. For Nicotine, standard solutions were prepared in water, and absorbance was measured at various concentrations (5-30 µg/ml) using the same method [24].
Formulation development
Fabrication of Naltrexone HCL and Nicotine MNs
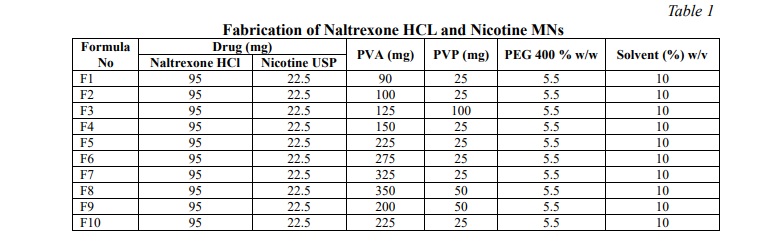
Naltrexone HCl and Nicotine microneedle (MN) patches were prepared using micro-molding techniques with varying ratios of PVP K30, PVA, and 5% PEG 400, as outlined in Table 1. Naltrexone HCl was dissolved in a phosphate buffer (pH 7.4), followed by the addition of PVP and PVA in different proportions. The mixture was sonicated for 1.5 hours to ensure dissolution. This solution was then added to a Polydimethylsiloxane (PDMS) microneedle mold (6.25 cm², 15 x 15 array, 500 µm needle height, 200 µm needle base) and sonicated to remove air bubbles. After one day in a desiccator, a second layer of PVP, PEG 400, and Nicotine USP was added and dried in an oven for 6 hours to form the needles. The patches were backed with aluminium foil.
Fabrication of Naltrexone HCl and Nicotine USP Transdermal Patches
Standard patches were prepared by combining Nicotine, Naltrexone HCl, and polymers in the same proportions as used for the Nicotine-Naltrexone microneedle formulation. The resulting mixture was poured into a 10.5 cm diameter Petri dish and dried in an oven at 40°C for 8 hours. Once fully dried, the patch was cut into smaller sections, each with the same drug content and surface area (5.75 cm²) as the microneedle patches.
Evaluation of Naltrexone HCl and Nicotine USP Microneedle Patch
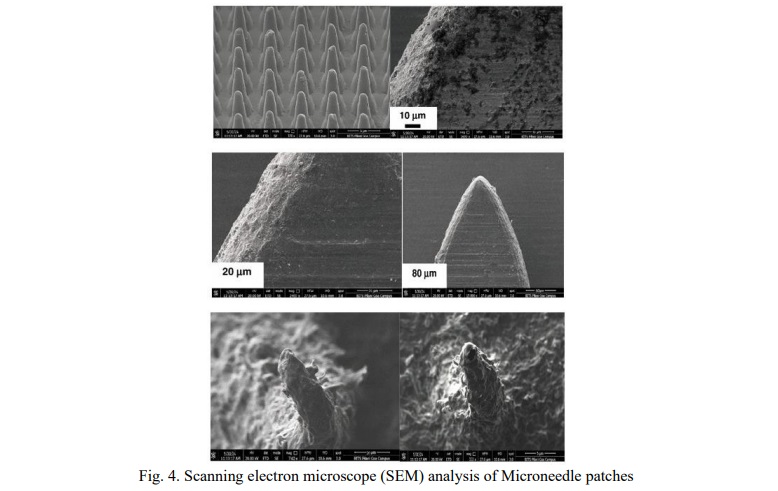
I. Scanning Electron Microscope Analysis: Microneedle patches were inspected for defects and analysed using a Quanta FEG 250 scanning electron microscope. Thin film samples were mounted on carbon-coated stubs and examined to assess needle size and morphology.
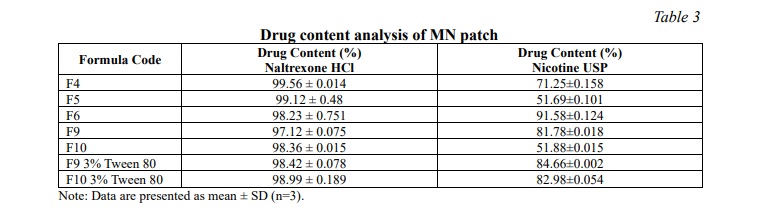
II. Drug Content Analysis: The patches were soaked in 25 ml of pH 7.4 phosphate buffer, followed by dilution and filtration. The absorbance was measured using a UV-visible spectrophotometer at the λmax for each drug. Drug content was assessed trice [24].
III. In-vitro Drug Release Studies: A mesh containing the patches was placed in a dissolution apparatus with 500 ml of pH 7.4 phosphate buffer, stirred at 50 rpm, and maintained at 35±0.5°C. Samples were withdrawn every 5 minutes for 1 hour to calculate the cumulative drug release. If 100% release were not attained by the end of the hour, 3% Tween 80 was added to the solution.
IV. In-Vitro Permeation Study: Using a Vertical Diffusion Cell apparatus, microneedle patches were tested in a cellulose acetate membrane setup [24]. The cell was immersed in a buffer solution at 37±1°C, with aliquots withdrawn periodically to determine drug concentration.
V. pH Measurement: The pH of the patch was measured by immersing it in 100 ml deionized water for 30 minutes and recording the pH with a meter, performed in triplicate.
VI. Uniformity testing: To ensure uniformity of weight and thickness, five patches were selected from each batch and weighed. Their thickness was then measured using a digital balance and Vernier callipers. The mean weight, thickness, and standard deviation were then determined.
VII. Statistical Data Analysis: Results are expressed as mean ± SD of triplicate samples. One-way ANOVA was used to assess statistical significance at P≤0.05.
Results
Preformulation of the powdered extract of the drug
Identification of the drug
The drug was examined for its physical characteristics, including colour, odour, flavour, and taste as depicted in Table 2.
Melting Point
The melting point of Naltrexone HCl was found to be around 169˚C.
IR Spectroscopy
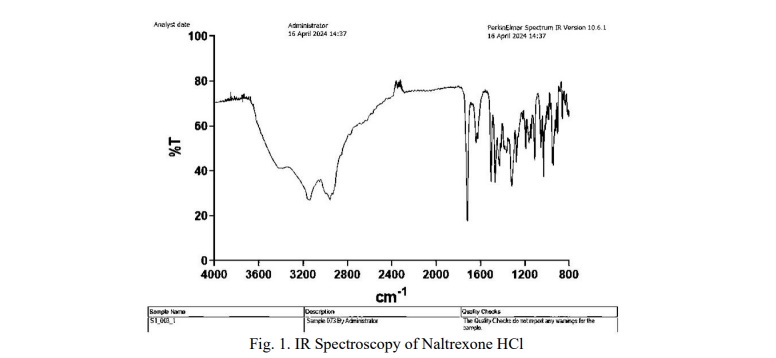
The IR spectrum of Naltrexone HCl shows key peaks at 1717 cm⁻¹ (C=O stretching), 1660 cm⁻¹ (C=C stretching), 1504 cm⁻¹ (aromatic ring), 1314 cm⁻¹ (O-H bending), and 1274 cm⁻¹ (C-O-C stretching) (Fig. 1).
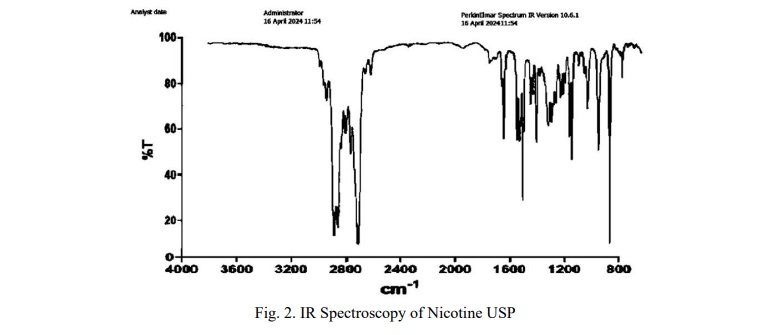
The IR spectrum of Nicotine USP displays peaks at 3300-3500 cm⁻¹ (N-H stretching), 2800-3000 cm⁻¹ (C-H stretching), 1500-1600 cm⁻¹ (C=C stretching), 1200-1400 cm⁻¹ (C-N stretching), 1370-1450 cm⁻¹ (CH₃ bending), and 700-900 cm⁻¹ (C-H bending) (Fig. 2).
The PXRD pattern for Naltrexone HCl exhibited well-defined and characteristic peaks. Three strongest and most characteristic low-angle reflections with intensity below 100 were observed approximately at around 6.5° 2θ (approximately 90-100), 8° 2θ (approximately 95-100) and 10° 2θ with an intensity of approximately 90-95 (Fig. 3).
Physicochemical Tests
For Naltrexone HCl, the water content was assessed using the loss on drying method. The resulting moisture content was 7.3% w/w, which is below the acceptable limit of not more than 12%. The weight of the ash obtained was 0.09 g, yielding a total ash content of 2.00% w/w.
Development of Analytical Method and Validation
Solubility test
Various solvents were used to evaluate the solubility of Nicotine USP. It was found to be highly soluble in water, ethanol, and glycerine, slightly soluble in propylene glycol, and insoluble in acetone. Naltrexone HCL showed high solubility in water and phosphate buffer at pH 7.4, slight solubility in ethanol, methanol, and isopropanol, and was insoluble in acetone and chloroform.
Determination of λmax by UV-Visible Spectroscopy
The λmax values for the drugs were measured using UV-visible spectroscopy. Nicotine USP had a peak absorbance at 261 nm in water (1.092) and 260 nm in phosphate buffer pH 7.4 (1.032). Naltrexone HCL exhibited a λmax at 203 nm in water (0.602) and 204 nm in phosphate buffer pH 7.4 (0.498).
Evaluation of Naltrexone HCl and Nicotine USP Microneedle Patch
Microscopic and visual inspection
Scanning electron microscope (SEM) analysis
Formulas F1, F2, F3, F7, and F8 failed visual inspection due to their high polymer viscosity, which hindered mold filling via vacuum application. The remaining formulas showed clear needles, as seen in Fig. 4.
Drug Content Analysis
Table 3 shows the mean percentage of drug content in the MN patches, which were found to be within acceptable limits.
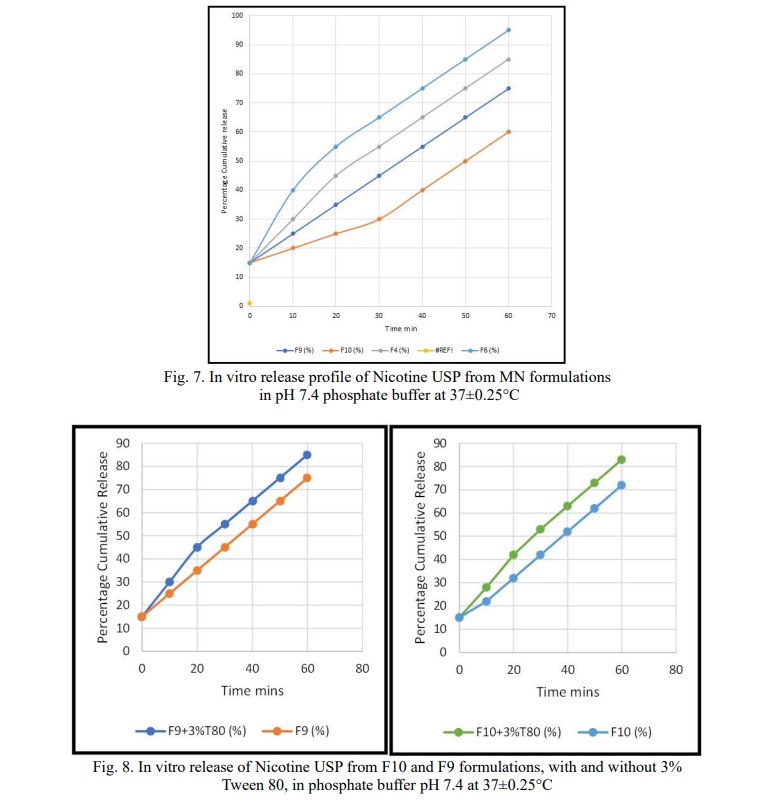
In-vitro drug release studies
Figure 3 shows the in vitro cumulative release of LXM at various time points. Formulas F4, F5, and F6, which formed successful MNs, achieved 100% release within 60 minutes (Fig. 5 and 7). Higher PVP ratios enhanced release speed by creating holes in the MNs, facilitating faster dissolution. This is due to PVP's hygroscopic properties, which increase moisture absorption and accelerate drug release.
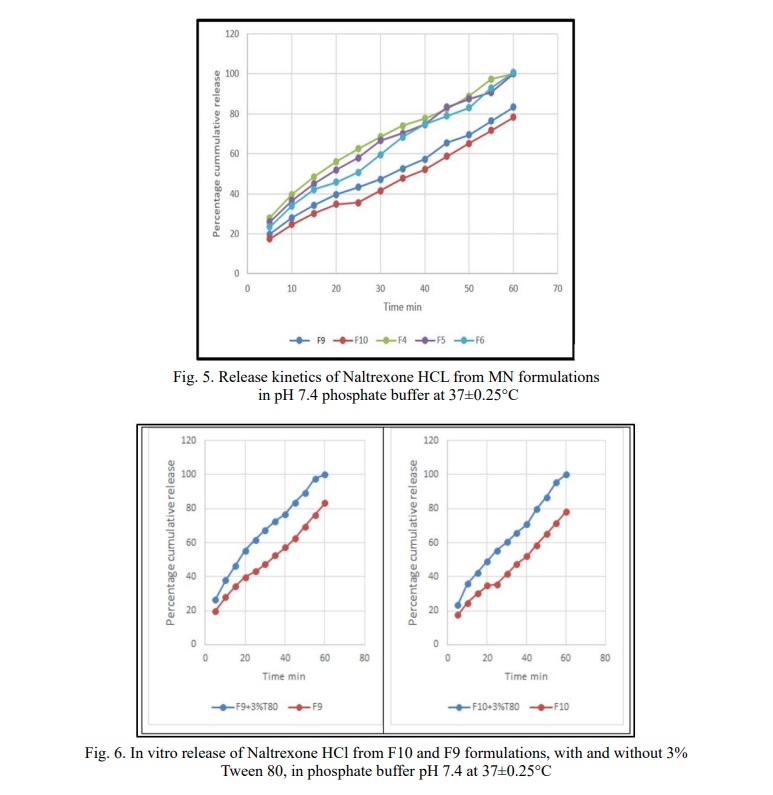
In contrast, F9 and F10 showed 78% and 83% release, respectively, within 1 hour due to a lower PVP ratio. Tween 80 was added at a 3% w/w concentration to both F9 and F10 to improve drug release, achieving 100% release as shown in Fig. 6 and 8. Tween 80 improved the dissolution rate by reducing interfacial tension, increasing polymer wetting and erosion.
In-Vitro permeation study
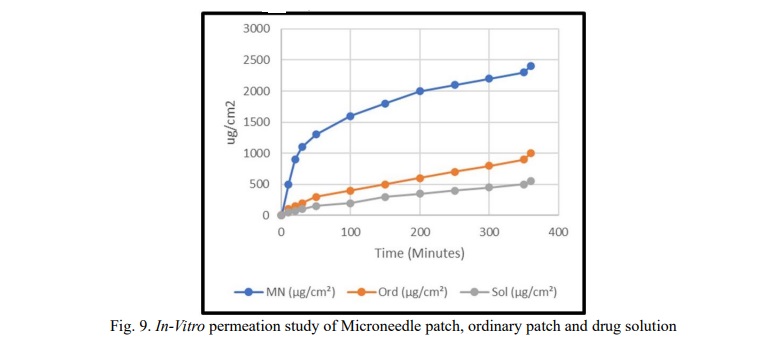
The microneedle patches of F10+3% T80 showed the highest cumulative drug permeation, reaching 67% over 6 hours, compared to 24% for the ordinary patch and 19% for the Naltrexone HCl and Nicotine USP solution. The steady-state flux rate (ssfr) was 3.98 µg/cm²/min for the MN patch, 1.46 µg/cm²/min for the ordinary patch, and 1.27 µg/cm²/min for the solution, demonstrating the MN patch's superiority with a 3.1-fold increase in flux rate compared to the LXM solution.
The MN patch exhibited the shortest lag time of 10 minutes, while the ordinary patch had a lag time of 50 minutes (Fig. 9). Although the drug solution showed faster initial permeation than the ordinary patch, its total cumulative drug release was lower. This is likely due to the surfactant and solubilizing effects of PVA and PVP in the ordinary patch, which facilitated higher drug permeation.
Kinetics of permeation
The kinetics of drug release for the formulations were analyzed using the DD Solver Excel add-in, where R2 values were calculated for the zero-order, first-order, and Higuchi models. Additionally, the n value for the Korsmeyer-Peppas model was determined. For formulation F4, the highest R2 value was obtained for the first order model at 0.9885, followed by 0.9739 for the Higuchi model. For formulation F5, the highest R2 value was obtained for the zero-order model at 0.9907, followed by 0.9537 for the Higuchi model. For formulation F6, the highest R2 value was obtained for the zero-order model at 0.997, followed by 0.9305 for the Higuchi model. For formulation F9, the highest R2 value was obtained for the first order model at 0.9928, followed by 0.9303 for the Higuchi model. For formulation F10, the highest R2 value was obtained for the zero-order model at 0.9922, followed by 0.9032 for the Higuchi model. The n values from the Korsmeyer-Peppas model indicated anomalous (non-Fickian) transport mechanisms for all formulations.
pH Measurement
The pH of the chosen formula was measured at 7.7±0.2.
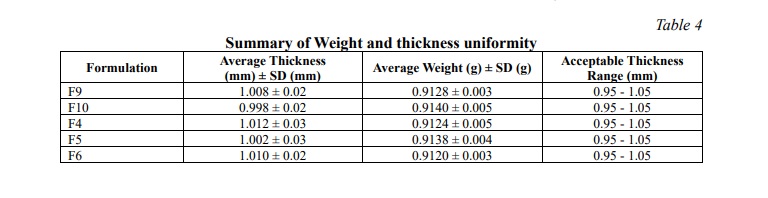
Weight and thickness uniformity
The thickness of five randomly selected patches from each batch was measured at five points using a Vernier caliper. The average thickness (1 mm ± 3%) and standard deviation were calculated, with batches showing variations greater than ± 5% being discarded. The mean weight of the patches was 0.913±0.043 g (Table 4).
Discussion. The preformulation study focused on identifying and characterizing Naltrexone HCl and Nicotine. Naltrexone HCl, a white crystalline powder, was odourless and bitter, with a melting point around 169°C, while Nicotine, a colourless to pale yellow liquid, exhibited a strong tobacco odour and turned brown upon exposure to air. FTIR analysis revealed characteristic peaks for Naltrexone HCl at 1717 cm⁻¹ (C=O stretching) and others, confirming its functional groups. Nicotine’s FTIR spectrum included peaks at 3300-3500 cm⁻¹ (N-H stretching) and others, validating its chemical structure. PXRD confirmed Naltrexone HCl’s crystalline nature with distinct peaks at 6.5°, 8°, and 10° (2θ). Physicochemical tests showed Naltrexone HCl with 7.3% moisture content and 2.0% total ash content, ensuring stability and purity, while Nicotine’s hygroscopic and volatile nature was noted.
The solubility tests showed that nicotine is highly soluble in water, ethanol, and glycerine, but insoluble in acetone. Naltrexone HCl demonstrated high solubility in water and phosphate buffer (pH 7.4), slight solubility in ethanol, methanol, and isopropanol, and was insoluble in acetone and chloroform. UV-Visible spectroscopy was used to determine the λmax values: nicotine showed an absorbance at 261 nm in water, while naltrexone HCL had λmax values at 203 nm in water and 204 nm in phosphate buffer, facilitating accurate quantification.
SEM analysis revealed issues with high-viscosity formulations F1, F2, F3, F7, and F8, while others showed clear needles. Drug content was within acceptable limits, with Naltrexone HCl ranging from 97.33% to 99.51% and Nicotine from 50.12% to 90.22%. Fast-release formulations F4, F5, and F6 achieved 100% release within 60 minutes due to high PVP ratios, while F9 and F10 with lower PVP ratios showed 78% and 83% release, respectively. Adding 3% Tween 80 improved drug release to 100% within an hour for F9 and F10.
In-Vitro permeation studies showed F10 with 3% Tween 80 had the highest cumulative drug permeation of 67% over 6 hours and a steady-state flux rate of 3.98 µg/cm²/min, compared to lower rates for ordinary patches and solutions. Kinetic analysis indicated first-order and zero-order release for F4, F5, and F6 with high R² values, and anomalous transport mechanisms for all formulations.
Optimized formulations F9 and F10, with lower PVP ratios and enhanced by 3% Tween 80, achieved 100% drug release in an hour and 67% drug permeation over 6 hours. Despite improved performance, these formulations failed stability tests, highlighting the need for proper storage conditions.
Conclusion. The research successfully optimized and characterized microneedle patches for transdermal delivery of Naltrexone HCl and Nicotine. Preformulation studies provided detailed insights into the physicochemical properties of the drugs, such as their solubility, thermal behaviour, and structural integrity, which were crucial for formulation design.
Among the tested microneedle patches, formulations F9 and F10 showed the best release profiles and drug permeation. Formulation F10, enhanced with Tween 80, demonstrated the highest efficacy by achieving 100% drug release within one hour and significant cumulative drug permeation in in-vitro studies.
Future research should focus on conducting extensive in vivo studies to further assess the efficacy, safety, and long-term effects of the optimized microneedle patches. Additionally, exploring variations in excipient ratios and drug concentrations could provide valuable insights into improving patch performance. To address stability concerns, the formulations should be subjected to rigorous stability testing under various environmental conditions. This includes optimizing storage conditions to minimize humidity and temperature fluctuations, and developing advanced packaging solutions to enhance product integrity and extend shelf life.
Financial support
No financial support has been provided for this work.
Thanks
The authors wish to express their gratitude to Mihir Virji (Nico Orgo) for generously providing a sample of nicotine for this research














Reference lists